We know the overview of how conduction works in the heart. SA node triggers action potentials which travel around the atria and bavk to the av node, where conduction slows (allowing atria to have time to contract), and then travels through the bundle of his and then the purkinje fibres to to ventricular muscle where contraction occurs.
We will look at specifically how the SA node generates constant changeable impulses.
The conduction cells in the heart are modified cardiomyocytes (modified as in no actin myosin etc), and so they have all of the Ltype calcium channel, SR, SERCA and PLN and all the other ion transporters. 2 things that are important are the funny sodium channels (which are voltage gated but open on hyperpolarisation instead of depolarisation), K channels that slowly lead to reduced K permanbility over time and T type calcium channels.
These all come together to give a resting membrane potential that is higher (closer to 0) than a typical cell, as well as a RMP that decays after depolarisation to trigger another. This is the “magic” of the SA node cells. The RMP decays leading to AP and depolarisation and is then reset to -60 mv, where it decays up to -40mv, Ap, depolarisation rinse repeat. It maintains a rhythm which can be altered with autonomic stimulation to serve what the body needs.
How does it do this? 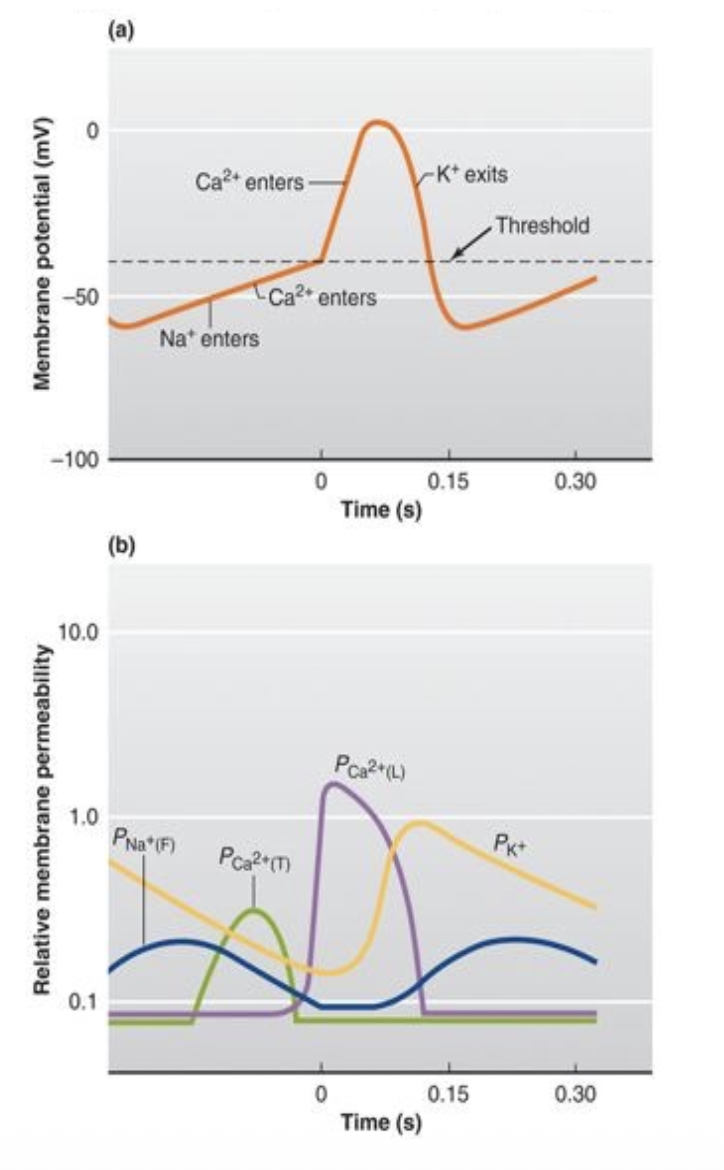
Lets start after repolarisation. Membrane potential is at lowest ~-60mv. This hyperpolarisation of the cell leads the funny sodium channels opening, letting positive Na+ into the cell, making it more positive. the K+ channels (which in this cell type closes late) are closing which means less positive moving out of the cell also making it more positive. these 2 factors lead to the “funny” current which is the decay of RMP to 0. About at -20mv the T-Type calcium channels open, leading to a final splash of calcium, leading to depolarisation. This causes the L-type calcium channels to open leading to massive calcium influx to the cytoplasm making it massively positive. The depolarisation also leads to K+ channels opening, which negatively hyperpolarises the cell back to point 1.
Autonomic control of heart rate.
The SA node has a natural frequency of about 100 BPM. Other conduction systems such as Purkinje fibres and AV node has slower natural frequencies but they are overridden by faster AV node (but still useful for backups). We do not always run at 100 BPM so something must slow it down.
The parasympathetic and sympathetic autonomic nervous systems alter the heart rate for higher (symp) or lower (parasymp) BPM.
Remember how Noradrenaline was able to increase calcium entrance and clearance rates, well Acetylcholine is able to decrease them. The mechanism is increasing or decreases the activity of adenyl cyclase via binding. this will increase or decrease cAMP which in turn alters PKA activity, which can then turnup or down all of our methods of calcium enterance and clearance, as well as other ions
Cardiomyocyte conduction 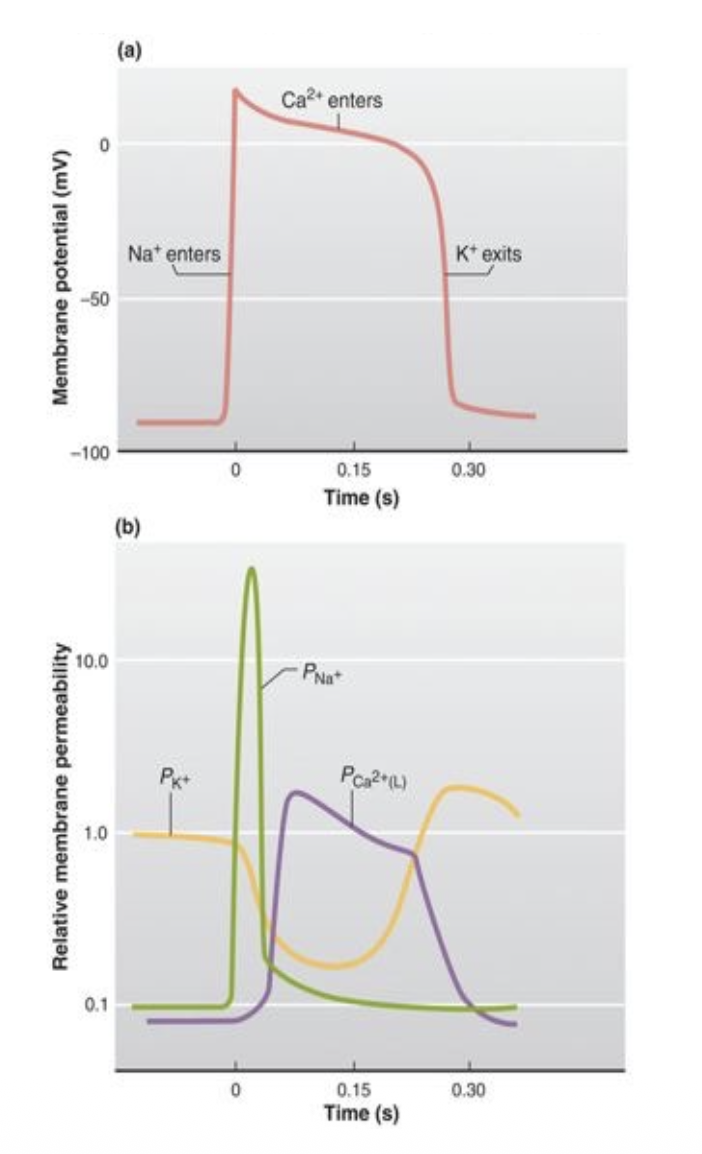
The action potential chart of the cardiomyocyte is the same as every other cell except for one thing, The massive calcium influx for contraction leads to massive plateau followed by increase K+ permeability for hyperpolarisation. Since its so long the electrical and mechanical activity overlap, making tetanus very very hard to do, which is good, we need the heart pumping not holding a position.