Fuels of the heart
The heart can use all fuels in the body: fatty acids, glucose, ketone bodies, lactate and amino acids. However it is highly oxidative and loves fatty acids the most. This in part is because fatty acids are the most energy dense fuel but also the most oxygen hungry fuel.
Recap of cellular metabolism
Carbs
Glycolysis breaks down glucose and glycogen into pyruvate and then inot acetyl CoA.
Fatty acids
these are broken down into acetyl CoA and H+ ions for the intermembrane space
Citric acid cycle
this turns the AcetylCoA into electron carriers
Oxidative phosphorylation
this decharges a whole bunch of elextron transporter to pump H+ and then uses the h+ gradient to turn AMP and ADP to ATP
Heart fuel use
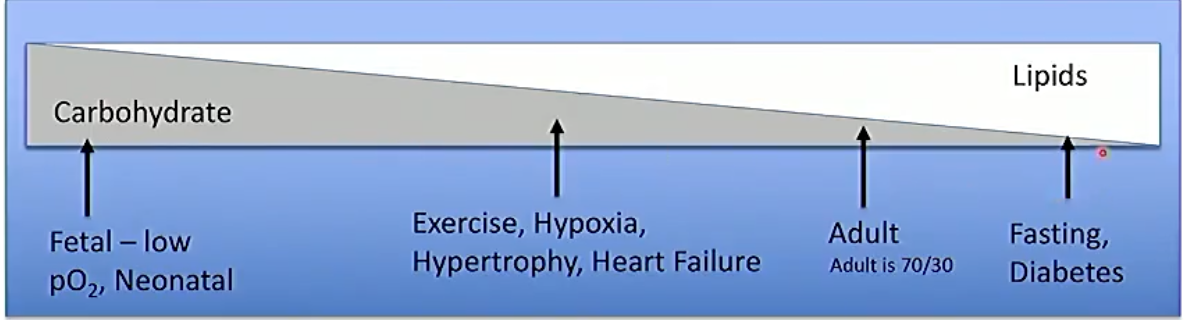
The heart can use different fuels based on different circumstances. It prefers lipids as they are so energy energy dense but will use carbohydrates if it is in hypoxic conditions.
Also limited access to resources will also alter the fuel usage of the heart, For example with diabetic it wont use sugars as it is unable to get them inside of the cell.
*“In a given situation fuel utilisation is modulated by many factors including:
- substrate availability
- hormones
- oxygen availability
- workload*“
Fuel transport
Glucose
Glucose gets into the cell via glut 1 and 4 receptors. Glut 1 is insulin independent and Glut 4 is insulin dependant. the glucose is phosphorylated to keep it in the cell.
Pyruvate can be made into lactate and release or it can be used.
Fatty acid metabolism
FFAs get into the cardiac cell be metabolised.
The rate of FFA transport into the mitochondria is inverse to the amount of acetyl-CoA this is becasue cytoplasmic ACC is turned into malonyl CoA and blocks entry of FFAs by binding to the FFA s transporters. High activity of CAC turns off PDH which stops glucose metabolism past pyruvate
Fed vs Fasting
Fed you are burning 50-75% carbohydrates 20% lipids. Fasting you are burning 80% lipids 20% carbs
Substrate use and disease
| State | Consequence |
|---|---|
| Diabetes | more FA oxidation and less carb oxidation as less carb transport into cell |
| Hypertrophied heart | more oxygen requirments lead to less FA oxidation and more Glycolysis |
| Ischaemic heart (Flow dependant) | Less oxidative metabolism more glycolysis |
| Hypoxic heart | Less oxidative metabolism more glycolysis\ |
| Reperfused heart | More FA oxidation Less carb oxidation Normal glycolysis |
Type 2 diabetes
In type 2 diabetes we see dysfunction of insulin receptors and getting glucose into the cell so we rely on FAs more. high relyance of FAs turn off glucose even more though PDH as well as turning down insulin receptors, leading to further challange.
Ischaemia
Ischaemia leads to more AMP which activates AMP kinase which downregulates acetyl coa carboxylase, this leads to less malonyl COA means more FFAs used in the mitochondria. This burns though oxygen leading to less ACC in the mitochondia turning on PDH more and leading to enourmous amounts of acetyl coa and malonyl coa
Hypoxia inducible factor is a transcription factor which upregulates carb metabolism
in high oxygen the HIF1 is oxidised and marked for destruction,
Exercise is cardioprotective
Footer
Associated lecture learning objectives:
- Know the fuels utilised by the heart
- Refresh your knowledge about the pathways generating ATP
- Be familiar with the swithcing of fuels in carious physiological and disease states
- Be familiar with some of the regulatory points involved in fuel switching
- Be familiar with the cardioprotective role of exercise and AMPK
Relevant lectures: Other links in medwiki: Comments: