Chronic Obstructive Pulmonary Disorder is a spectrum of disease ranging from chronic bronchitis to Emphysema. Both are permanent and often occur together, albeit one more so than the other. But treatment and easing of some symptoms are still possible.
Emphysema
Emphysema is where the alveoli and the bronchioles are damaged and the connective tissues destroyed.
Pathogenesis
The destruction of the lung tissue is often due to cigarette smoking. The cigarette smoke produces oxidants and leads to ongoing accumulation of inflammatory cells in the lungs. oxidant and proteolytic enzymes (elastases mostly) released from inflammatory cells destroy elastic tissue in the alveolar walls. Smoking also inhibits the alpha-1-antitrypsin. All of this results in Alveolar wall destruction.
Morphology
It can be centreacinar which involves the proximal airways and bronchioles this is most common as emphysema is most often due to smoking and the cigarette smoke does not reach all the way to the alveoli. Panacinar emphysema does affect the alveoli and alveolar spaces but not so much the proximal airways and bronchioles.
Bullous emphysema 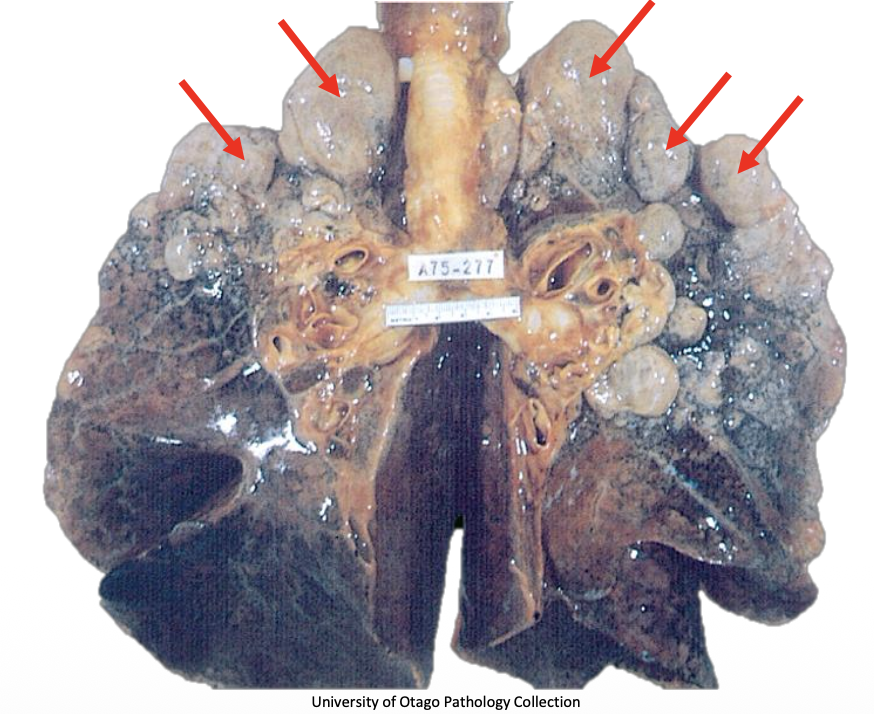
Bullous emphysema is when multiple dilates airspaces come together and create large bullae (bubbles)
Chronic bronchitis
This is a chronic state of inflammation in the lungs, clinically defined as perisitent cough with sputum production for at least 3 months in 2 consecutive years.
Pathogenesis
Chronic irritation or infect can lead to chronic bronchitis. The majority of time the causative irritant is cigarette smoke.
The cigarette smoke causes chronic inflammation in the bronchi and bronchioles. Chronic inflammation releases inflammatory mediators and growth factors which makes the bronchial wall undergo metaplasia of surface epithelium into goblet cells or squamous epithelium and hyper trophy and hyperplasia of mucous secreting glands.
This leads to mucous over production which may be a protective mechanism against smoke but obstructs the air way.
The obstruction leads to further infection which is exacerbated by smoking worsening the clearing ability of respiratory cilia.
Chronic bronchitis vs Emphysema
| Predominant bronchitis | Predominant Emphysema | |
|---|---|---|
| Age | 40-45 | 50-75 |
| Dysnpea | Mild and late in disease | Severe and early in disease |
| Cough | Early in disease, copious sputum | Late in disease, not much sputum |
| Infections | Common | Occasional |
| Respiratory insufficiency | Repeated | Terminal (?) |
| Cor pulmonale | Common | rare, Terminal |
| Airway resistance | Increased | normal or slightly increased |
| Elastic recoil | Normal | Low |
| Chest radiograph | Prominent vessels, large heart | Hyperinflation, small heart |
| Appearance | Blue bloater | pink puffer |
Blue bloater
Those with chronic bronchitis are often called blue bloaters, as the obstruction and inflammation in the lungs lead to increased resistance to blood flow. This in turn leads to right heart failure, leading to cyanosis and oedema. This is called cor pulmonale.
Pink puffer
People with emphysema are called this because they are often pink in the face from exertion of breathing as well as puffing, with pursed lips to avoid dynamic airway collapse from their reduced elastas