Intro to lung cancer
The cancers of the lung can be very deadly and also very preventable in most cases. The main cause of lung cancer is smoking.
Aetiology
Cigarettes
~80% of lung cancers occur in smokers. 11% of heavy smokers develop cancer so there are a number of factors involved as not all of them have cancer.
Risk factors
- Heavy smoking 2 packs a day for 20 years increases the risk 60 times
- Females are more susceptible to carcinogenic effects of smoking
- Second hand smoke doubles cancer risk for non-smokers
- Cessation for 10 yrs or more stops risk from increasing but the mutations are still there.
Asbestos
Asbestos is a famous cause of cancers of the lung fibrosis of the lung and mesothelioma (tumor of the pleura). MIning, construciton and demolition engineers and boiler maksers are at risk
Exposure to asbestos and smoking increses the risk of lung cancer greater than the individual risk factors added together
Pathogenesis
Cancer in the lung is like other cancers. It is the result of many mutations leading to transformation, The mutations can be from physical irritants, chemical carcinogens (smoking), etc.
DIfferent types of cancers have different mutations affecting oncogenes and tumour supressor genes
Lung cancer morphology 
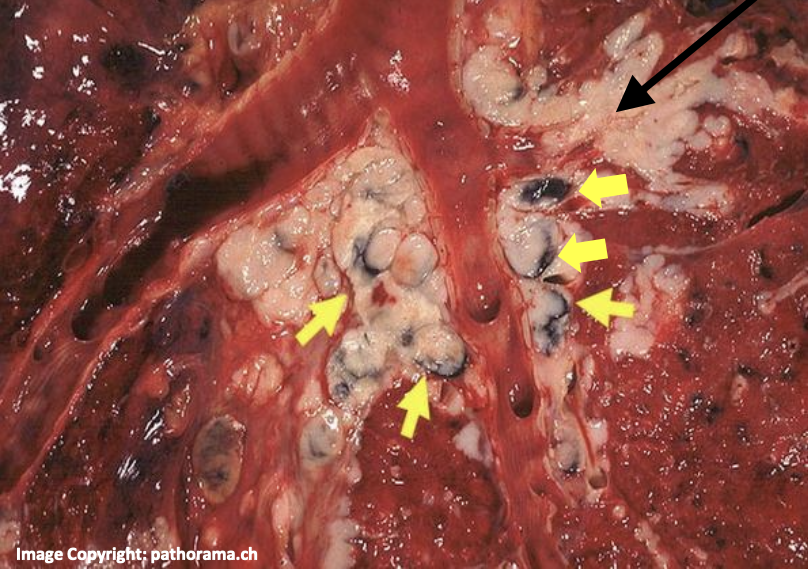
Lung carcinoma often is grey white, and firm to the touch. It is often speckled with carbon (anthracosis) and areas of haemorrhage and friable tissue necrosis can be seen in the tumour.
In the second picture you can see how the small cell carcinoma its clustered around the bronchial wall and (i cant see it personally) infiltrated the lymph nodes.
Growth patterns of cancer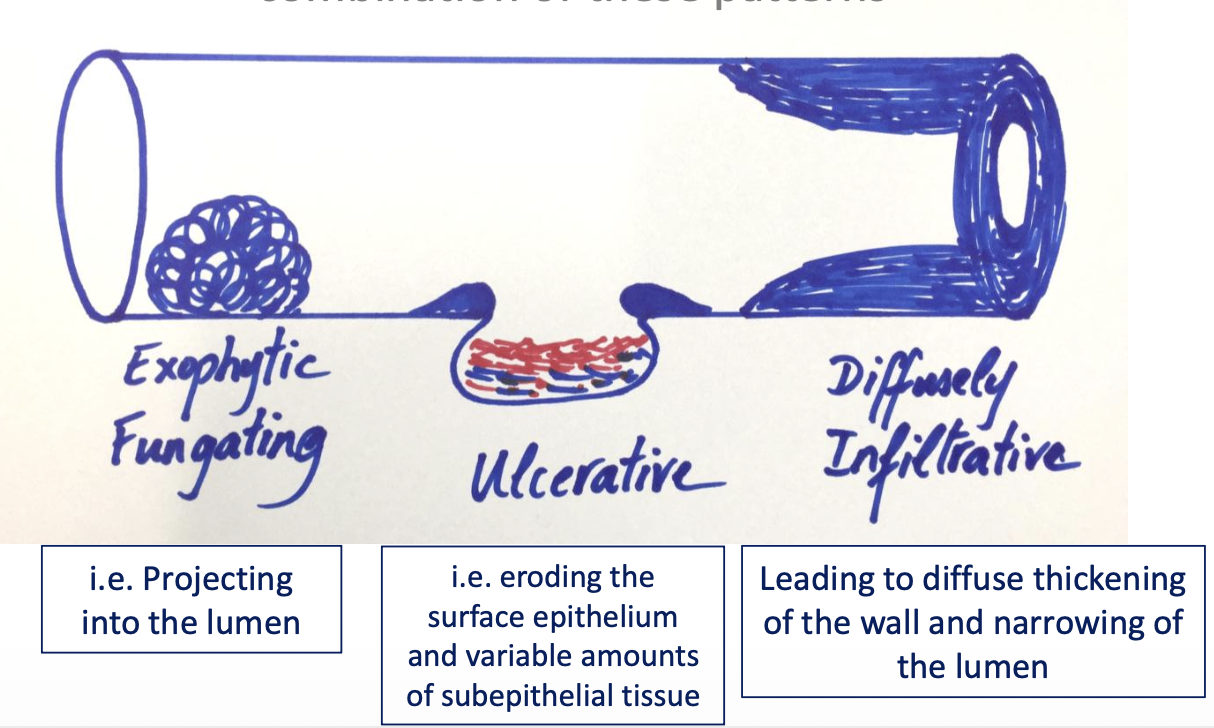
Cancer grows in a few different ways (not mutually exclusive). These are per the graph. Useful for describing pathological images (the tutorial).
Variants
This is a little more important and a little less common knowledge There are a few major variants of lung cancer and their differences stem mostly from the origin cells.
These are the variants:
Adenocarcinoma
This is a tumour that forms glands and can produce mucin. It had GOF mutations of oncogenes EGFR and KRAS. Lest common cancer in smokers and most common in non-smokers and more in women compared to men.
More often peripheral under the pleura
Morphology
The microscopic morphology is lots of malignant irregularly sizes and shaped glands which is surrounded by fibrous tissue background. The tumour destroys normal lung architecture
Squamous cell carcinoma
Strongly associated with smoking High frequency of LOF mutations of tumour suppressor gene p53.
More often central and hilar
Morphology 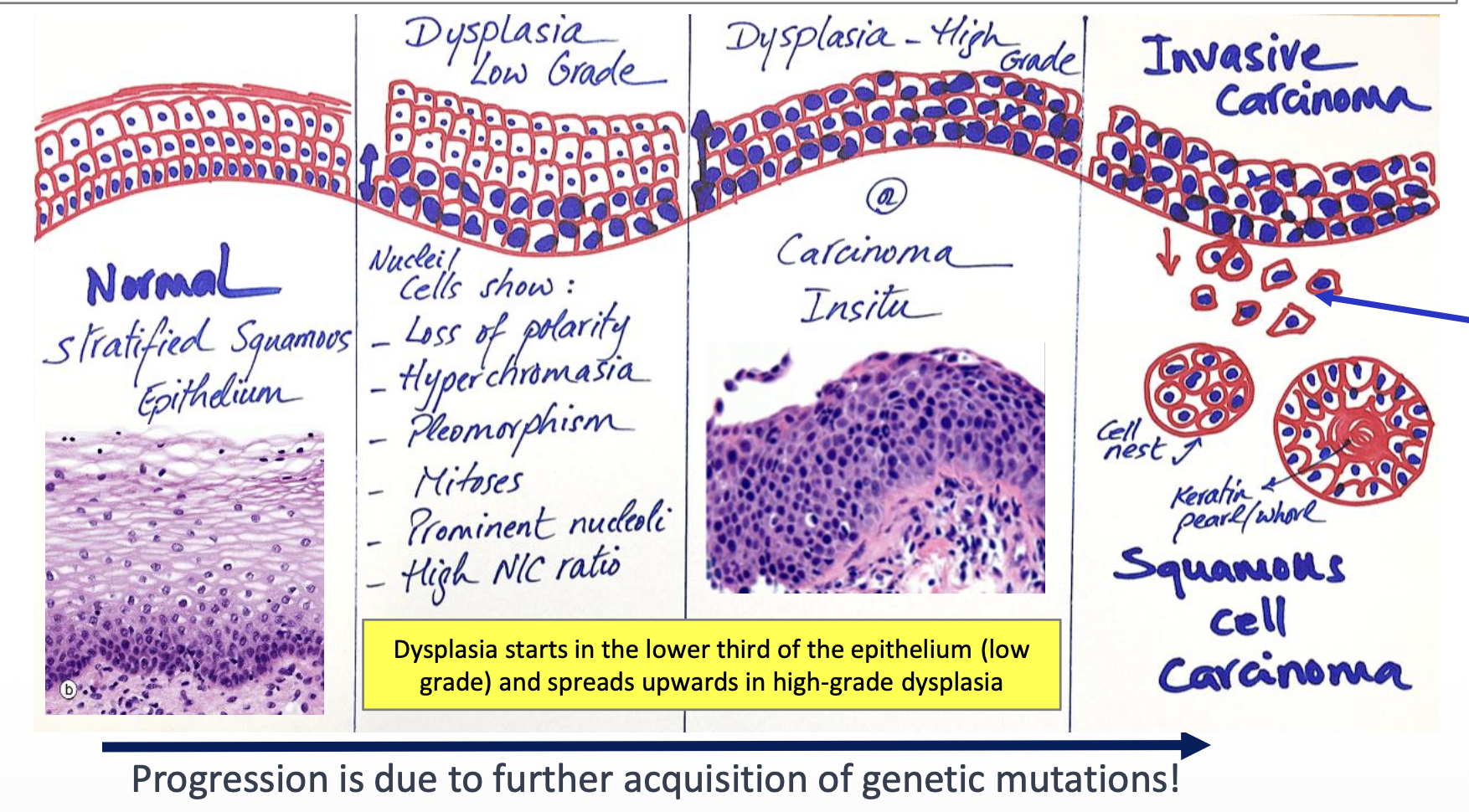
This is a shift of respiratory epithelium to squamous epithelium and then transformation. This is an example of hyperplasia → metaplasia → dysplasia (while dysplasia isnt cancer in itself it is a premalignant change)
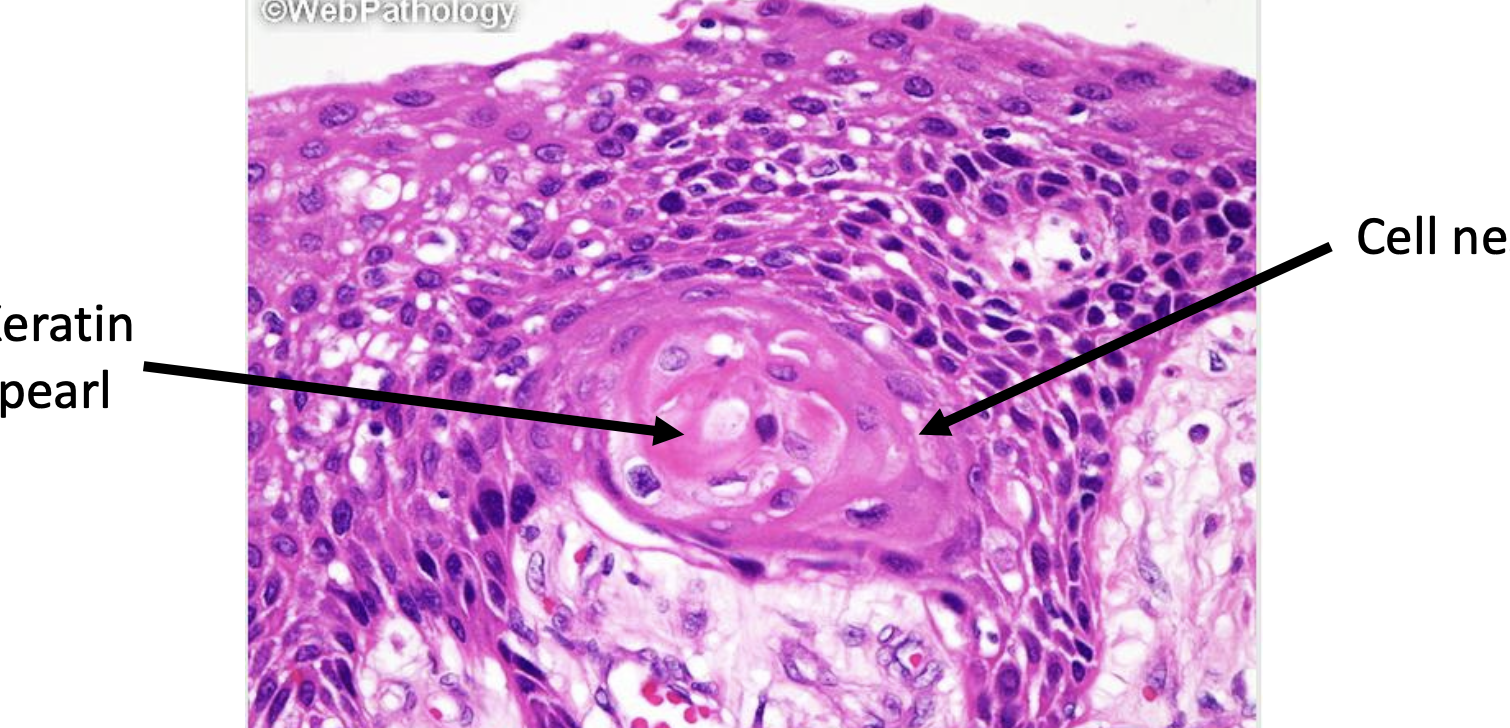
Additionally in well differentiated SCCs malignant tumour cells are arranged in groups called cell nests with central keratinization called keratin pearls or whorls
Another feature of SCC is intercellular bridges (dunno if they are uses ad brindges they just look like perpindicular strands) (click on image for magnification)
Small cell carcinoma
Strongest association with smoking. Highly malignant and show mutations of p53 and BCL2 antiapoptotic gene. More often central and hilar in the lung
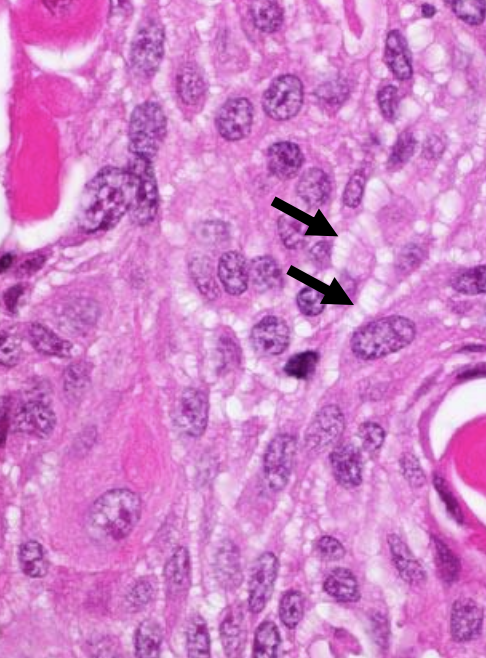
Morphology 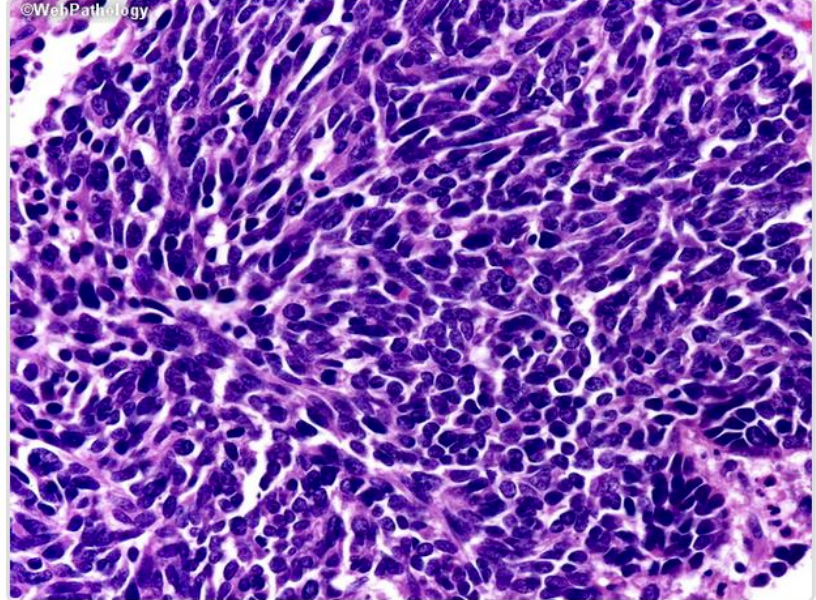
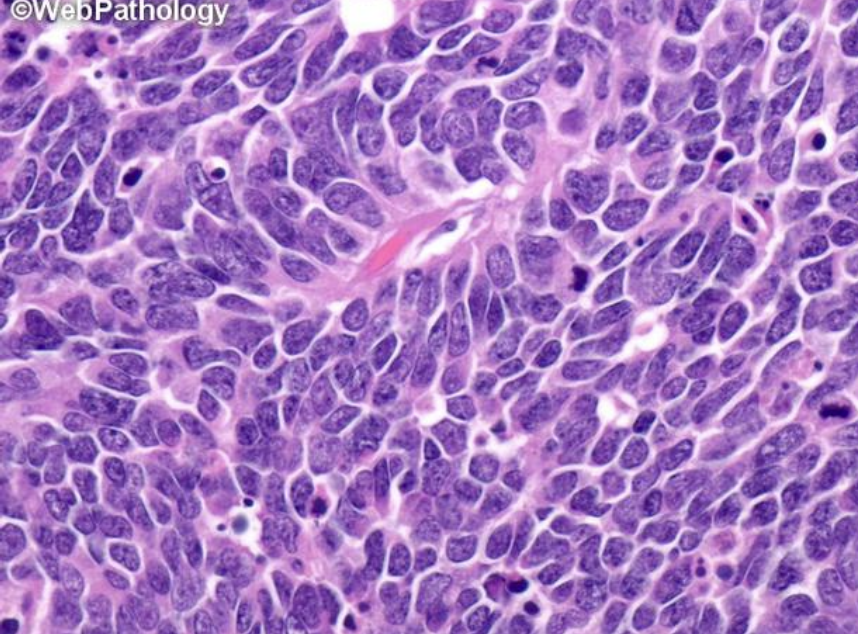
This tumour arises from neuroendocine cells in the bronchial epithelial lining. It has no precursor lesions. The tumour cells are small with little cytoplasm, but darks hyperchromatic nuclei with finely granular chromatin. Additionally nuclear moulding is present, where the nucleus mould to cell shape
Large cell carcinoma, and others
Clinical
Presenting complaints
The main presenting complaints are cough, sometimes with haemoptysis, chest pain, dyspnea and weightless (cachexia). Often the tumour may be discovered after metastasis
Some investigations that can be done are:
- Chest X-ray
- Sputum cytology
- Imaging: ct, MRI
- bronchoscopy
- Tissue biopsy or cytology
Treatment
There are several treatment modalities
- surgery
- chemo
- radiation
- new novel therapies (immunotherapy against EGFR receptors in adenocarcinomas for example)
Small cell lung cancer treatment is very different from other cancers so much so treatment is classified into small cell lung cancer and non small cell lung cancer.
Adenocarcinomas and SCC are still localised on diagnosis and can be cured by surgicall excision by a lobectomy operation
SCLC his usually metastatic on presentatio and is highly sensitice to radiation therapy and chemo.
Prognosis is slim for lung cancer with 5 yr survival being only ~16%
Paraneoplastic syndromes
This is where there is signs and symptoms that cannot be explained by local spread or metastasis of the cancer or disturbances from the cancer. Paraneoplastic syndrome could be hormones secreted from a gland or immune activation to a new tumour antigen. However the cause is not often known.