Pneumonia is the inflammation of lung tissue usually from an infectious organism. Pneumonia can be classified by clinical setting (community acquired, aspiration), organism (mycoplasma pneumococcal) or morphology (lobar or bronchopneumonia) and different organisms are associtated with different classifications.
Predisposing risk factors
Most of the risk factors for pneumonia are all in common with things that reduce the ability to clear infection or secretions physically out of the lungs:
- Decreased cough reflex: the less you can effectively cough the worse you will be at clearing stuff in the lungs out.
- Injury to cilia: things that disable cilia make it harder for the body to clear secretions
- Decreased function of alvoelar macrophages (smoking): this can make it harder to fight infections in the lings
- Oedema or congestion: wet soggy lungs promote bacterial spread
- retention of secretions (many causes, specific example is thick mucous that is harder to clear in CF patients)
ARDS 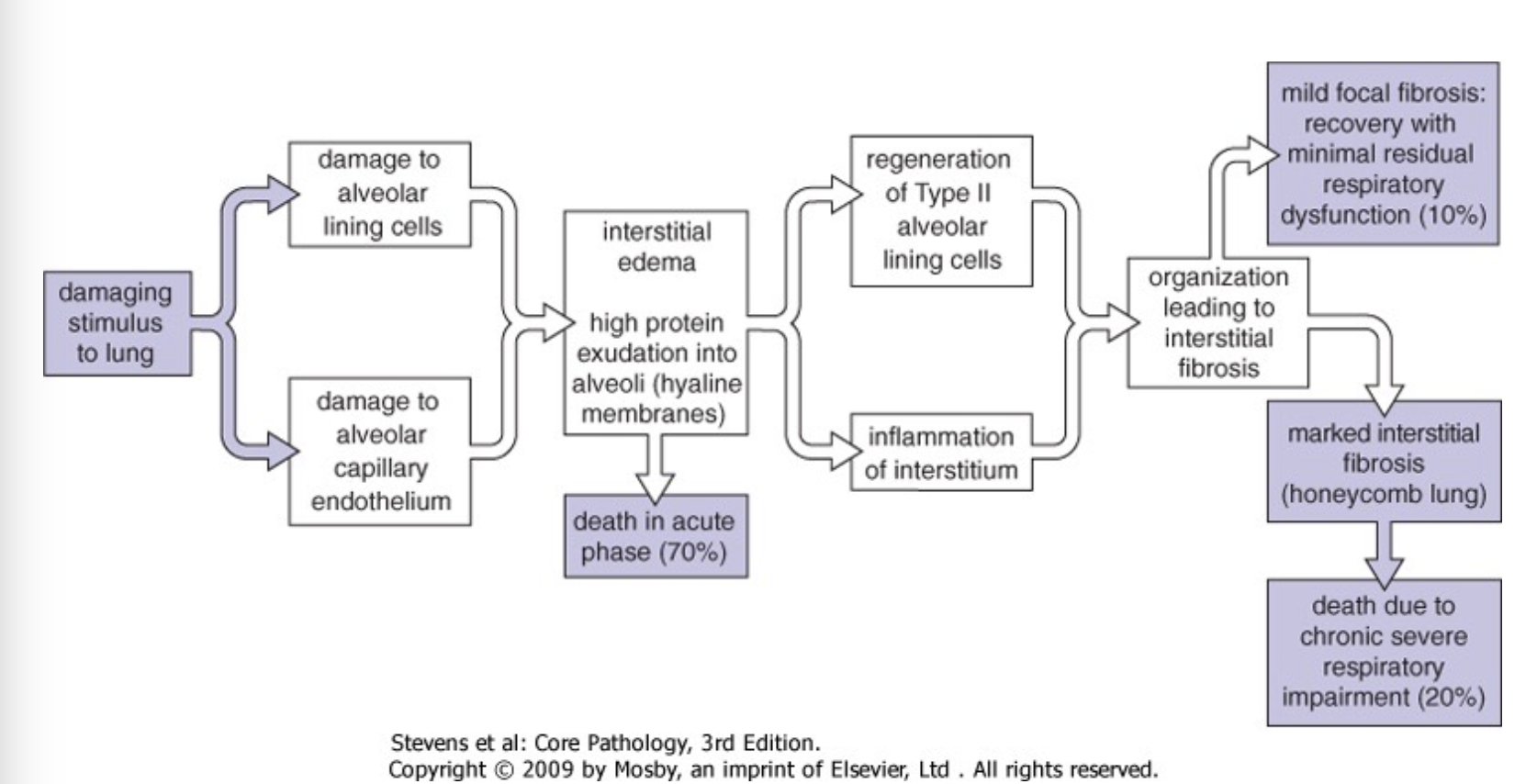
This is a respiratory syndrome which can happen from injurious stimuli. It can happen from a number of causes one of which is pneumonia but it could be caused by tuberculosis too or something. The lecture mainly describes what happens during this and its outcome but this is touched on very briefly.
There are 2 phases to ARDS, the proliferative phase and the fibrotic phase. The proliferative phase lasts 1-3 weeks and is characterised by proliferation of type II pneumocytes and macrophages invade and remove cell debris.
The Fibrotic phase consists of resolution with minimal fibrosis. Repair happens here often with thing alveolar wall resulting as well as progressive fibrosis?
Micromorphology 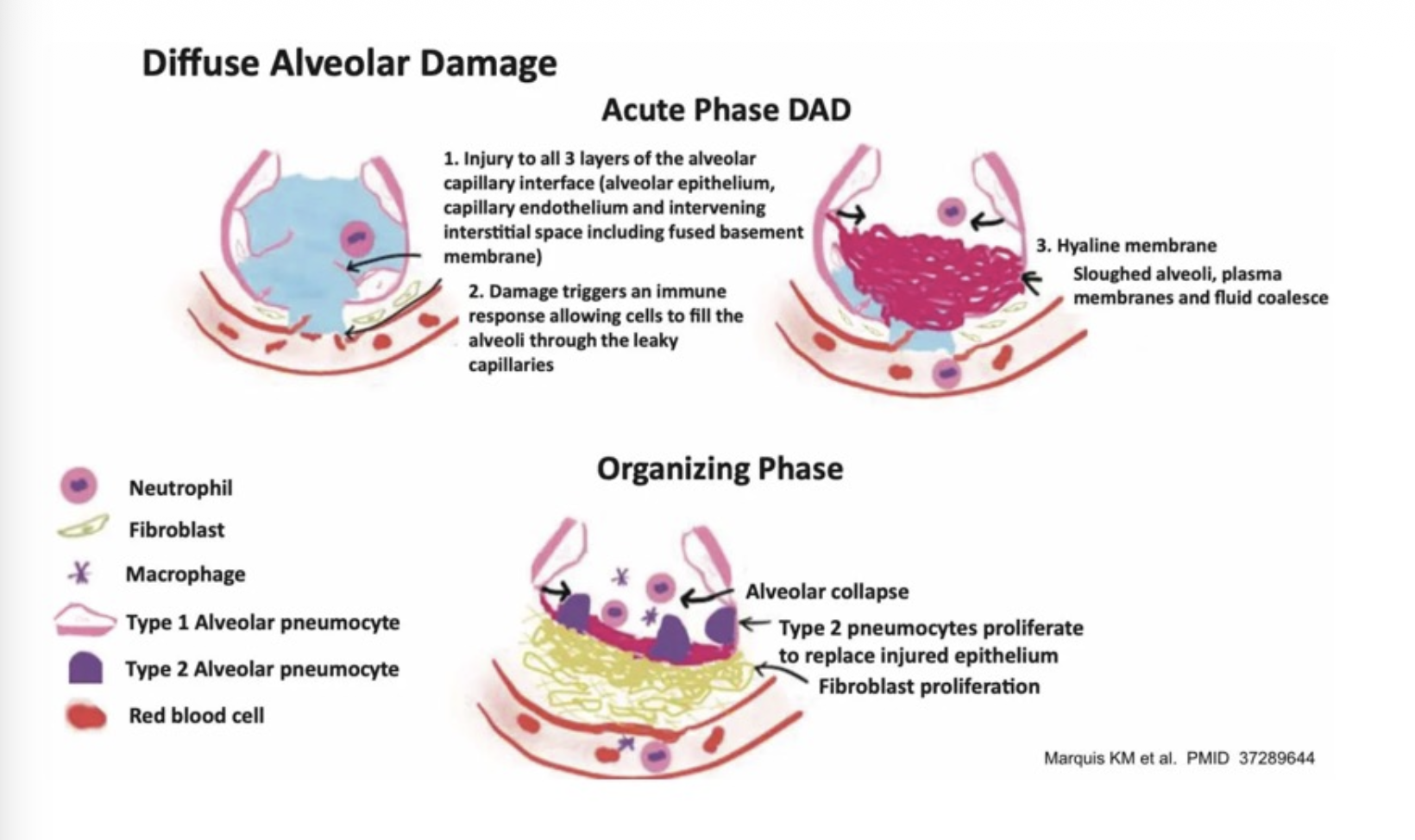
Consult the adjacent image after consulting the above graph
Bacterial pneumonia
Bronchopneumonia
This is where the main method of spread it though the bronchi and bronchioles and so we see spots of pneumonic consolidation at certain alveolar dead ends. I think that the lower aleovi are more effected due to pus carrying bacteria downwards
Lobar pneumonia (lobe-ar)
This is when a lobe is effected and it is “confluent consolidation involvinfing a complete lung lobe infection through pores of Khon”. this means all the alveoli have been infected within a lung
Clinical settings
This is unsually community acquired and classically occurs in otherwise healthy young adults.
Pathology
Pathology is a classical acute inflammatory response, with exudation of fibrin rich fluid, neutrophil infiltration, macrophage infiltration and resolution. Immune system helps with antibodies leading to opsonisation with phagecytosis of bacteria
Stages of lobar pneumonia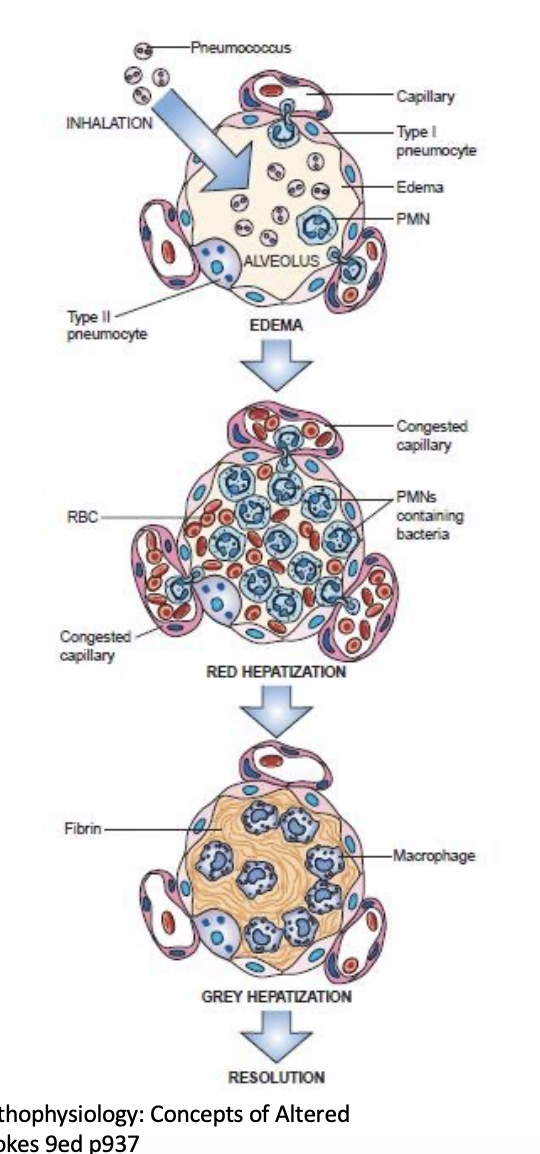
These stages are congestion, red hepatisation grey hepatisation and resolution. All of these are visually different and help with identifying what is going on with the lungs.
Congestion
This is where the capillaries are congested and the lung becomes oedematous
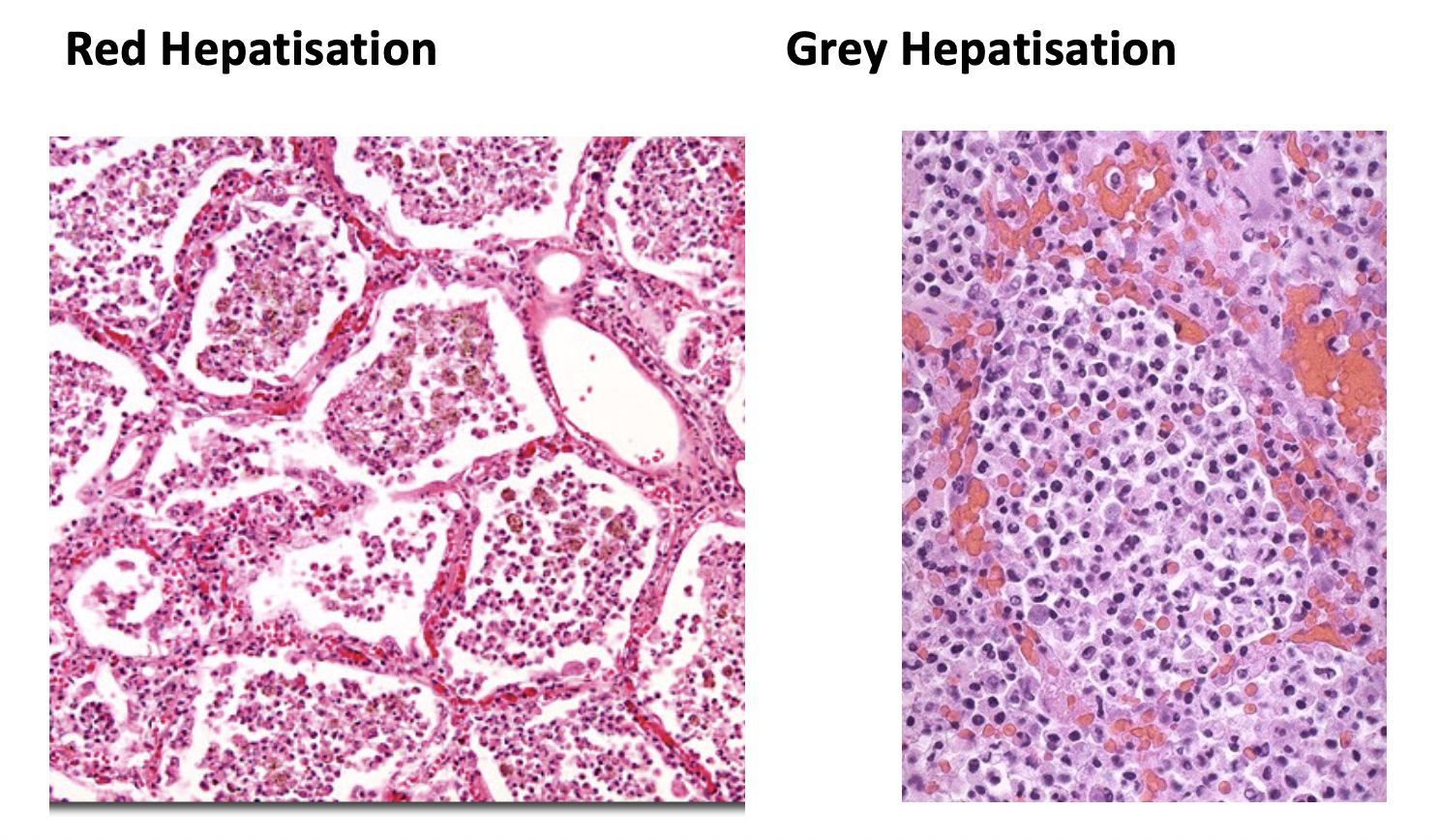
Red Hepatisation
This is where the red cells enter the alveolus (bleeding into the lung). Neutrophils also enter the lungs and ingest bacteria,
Grey Hepatisation
This is where macrophages ingest and remove deas inflammatory cells and fibrinous exudate.
Resolution
All is well if not with a bit more scarring
Microscopic appearances
Bronchopneumonia
Bronchopneumonia is patchy and not confined by lobar architecture yet. It mainly spreads through airways.
Often can happen along with;
- Post-viral state: Viral infections regear and weaken the immune system.
- Depressed cough reflex: Clearing secretions. See above
- Distal to obstruction: Clearing secretions. See above
- Aspiration: stuff in lungs can lead to infections
- Immunosuppression: …
- Cardiac failure: pulmonary oedema
Viral pneumonia 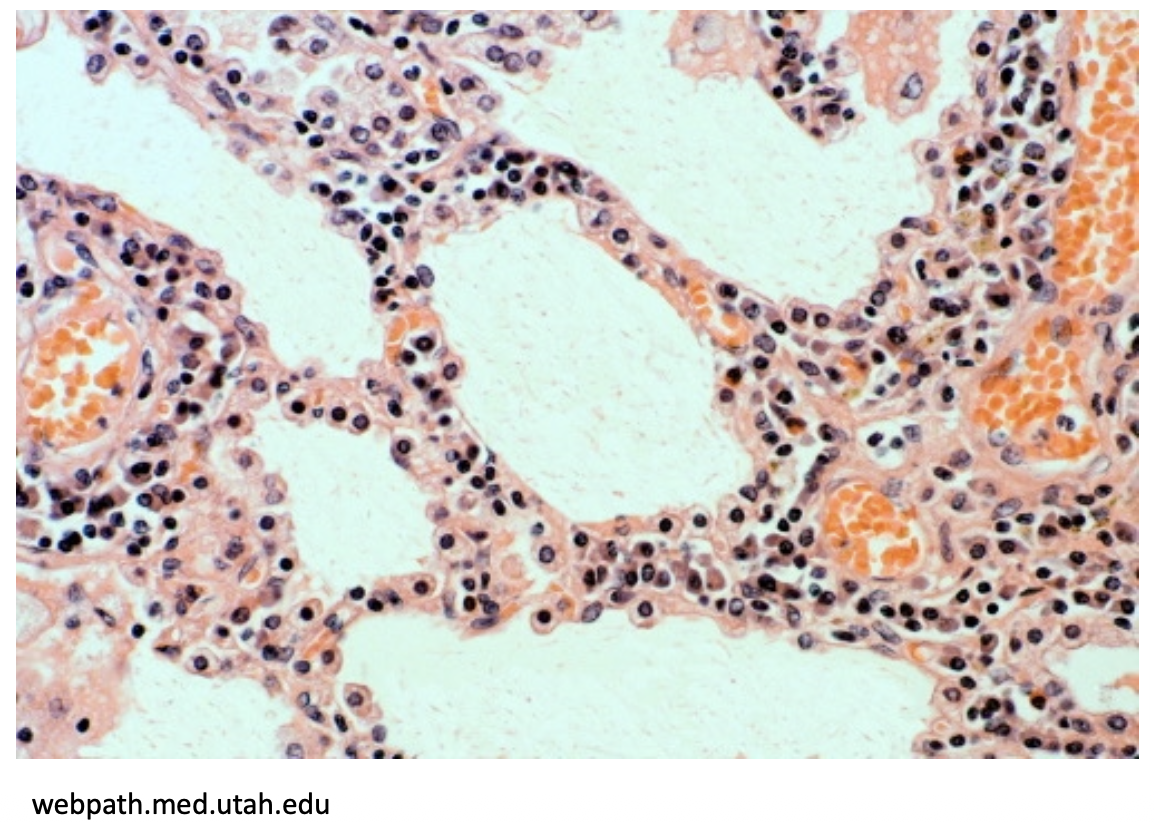
This is where there is a viral infection in the alveolar walls. As seen in the adjacent image the macrophage and lymphocyte influx in into the alveolar wall, as that is where the viral infection is.
However later viral pneumonia has an ARDS like injury pattern. acute inflammatory infiltration is lass obvious.
Some causes are:
- Respiratory syncytial virus
- measles pneumonia
- covid pneumonia
- Influenza pneumonia
Immunocompromised hosts
We see more “exotic” infection that would not be usually found in these patients with causes of pneumonia like
- Cytomegalovirus
- Mycobacterium avium intracellulare
- Aspergillus, candida, pneumocystis
- Cryptosporidia, toxoplasma