Rheumatic fever
Rheumatic fever is a significant condition that has long lasting effects. It is an acquired autoimmune condition where after and infection of streptococcus pyogenes, the body thinks that proteins in your heart are foreign and mounts an immune response to them.
Pathogenesis
Rheumatic fever arises when the body recognises the self. This can occur when there are repeat infections of Group A Streptococcus (streptococcus pyogenes) in the skin or throat, as these produce a protein called protein M which is what the body forming antibodies to, that are cross-reactive to proteins in your heart.
Often rheumatic fever occurs well after the infection to the body has resolved. We See the cross reactivity manifest as pancarditis (inflammation of all 3 layers of the heart)
Signs and Symptoms
- Monoarticular pain
- fatigue
- Pericardial rub on auscultation of the heart
Complications
As rheumatic fever builds acute inflammation occurs in the heart where vegetations of platelets form and eventually subside (but could be infected while still existing see Infective endocarditis).
Management
Related stats about vulnerable groups and risk factos
This is a disease of poverty and thus we see Māori populations overpresented
Pathology
Morphology
We see pancarditis, infection of all 3 layers of the heart wall, endocarditis, myocarditis and pericarditis. In the endocarditis we inflammation of mural and valvular endocardium on the left side of the heart. Myocarditis can create soft and flabby myocardium leading to dilation of the heart chambers but mostly the left ventricle. Pericarditis, where a rub can be heard from the exudate and inflamed tissue on heartbeat.
Rheumatic Pericarditis 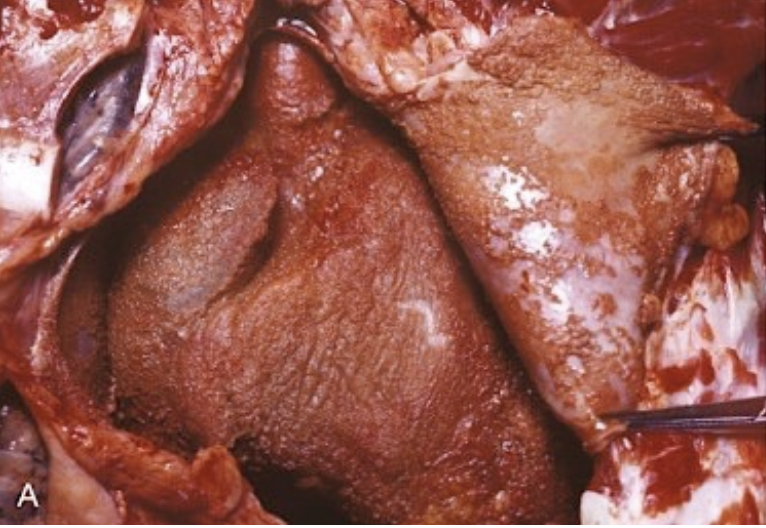
The inflammed surface has a layer of fibrinous exudate on it and is called bread and butter pericarditis
Rheumatic Myocarditis 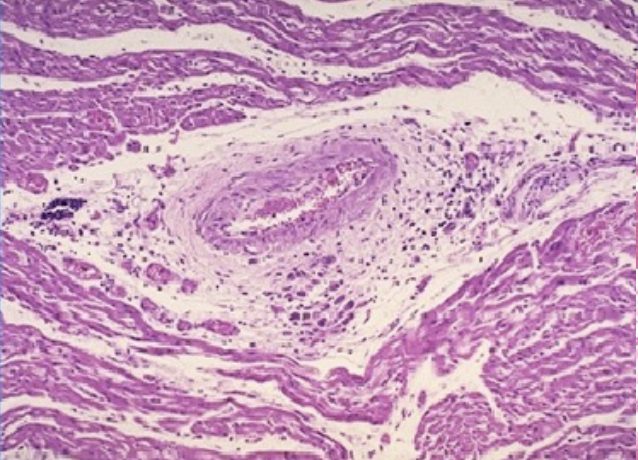
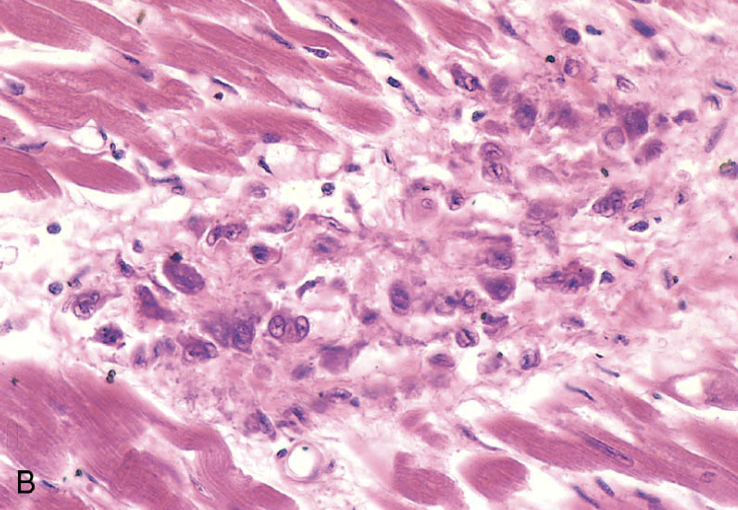
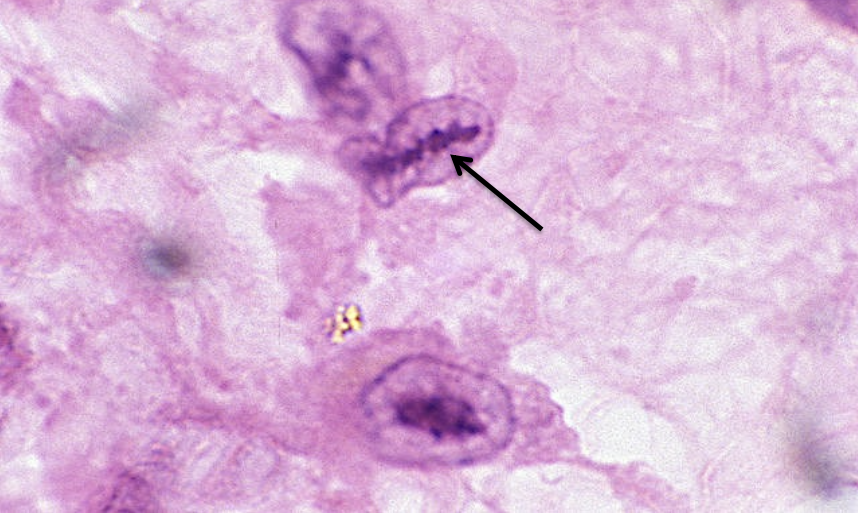
The foci of inflammation in the myocardium are called Aschoff bodies (See images) and are mode of central necrosis surrounded by lymphocytes (mostly T cells, plasma cells and activated macrophages called anitschkow cells. These cells have chromatin that is condensed into long wavy ribbons.(see image)
Rheumatic Endocarditis
Verrucae (sterile masses of antibodies, complement, fibrin and platelets) form in the lines of closure of the mitral valve
Rheumatic heart disease
This is where the heart is permanently damaged by Rheumatic fever, we see valvular diseases like stenosis, and regurgitation. This can lead to ventricular hypertrophy and chronic heart failure. The Mitral valve is the most effected valve usually.
Pathogenesis
Multiple episodes of rheumatic fever over time can eventually lead to RHD. Healing be fibrosis leads to permanent valve deformities.
Signs and symptoms
Complications
Chronic Heart failure after a long period of associated valvular disease
Management
Surgery (valve replacement), meds to lever blood pressure,
Pathology
Morphology: 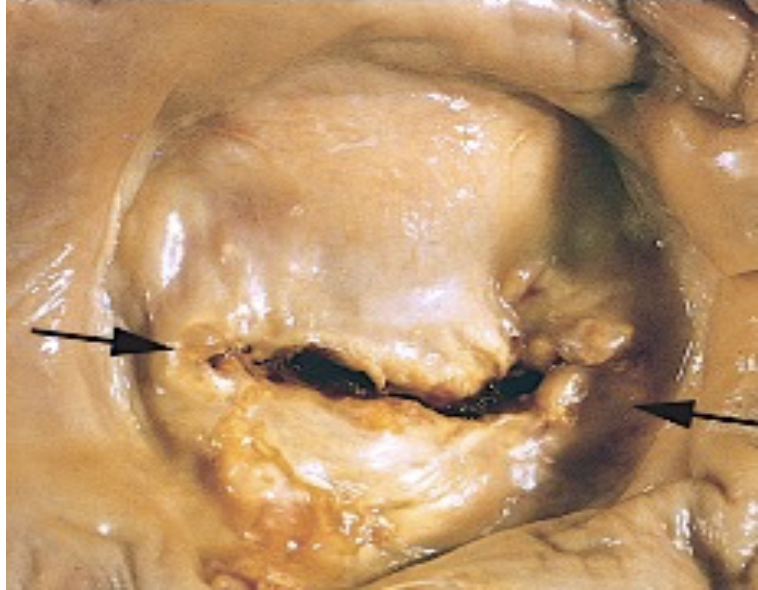
The scarring of the mitral valve (which is almost always involved) happens over repeat occurrences of RF and leads to fusion of commissures (the edges of the line which seperates the valve leaflets like the edges of your mouth). leading to a button-hole or fish mouth appearance.
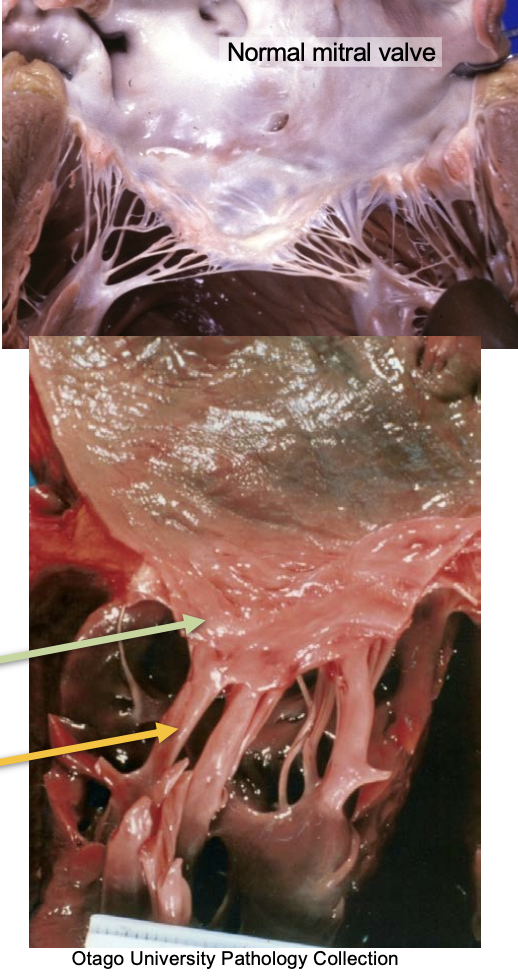
Additionally the chordae tenineae become shortened, thickened and fused. (See comparison on the right)
Footer
Relevant lectures: L08 valvular heart disease in Pathology Subjects involves: CVS, PATH, CASES Other links in medwiki: infective endocarditis, streptococcus pyogenes, Chronic heart failure, case 06 fainting Comments: